




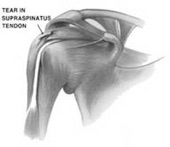
Rotator Cuff Tear
 Arthroscopic Picture of
Arthroscopic Picture of Rotator Cuff Tear
Rotator cuff tears remain one of the most common causes of shoulder pain and disability among adults. In fact, by the time one reaches the age of 60, there is a 50% chance of at least a partial tear of the rotator cuff. For those fortunate enough to have a painful rotator cuff tear, there is a 50% chance of having a silent rotator cuff tear in the other shoulder!
There are four tendons that make up the rotator cuff; however, the vast majority of tears occur in the supraspinatus tendon. With rare exceptions, tears of the supraspinatus occur at the attachment to the bone.
There are many causes of rotator cuff tears. Most commonly, degeneration of the rotator cuff and normal aging results in a weak tendon that can easily tear. Often, the patient cannot recall a specific event that may have caused the tear. In other cases, a specific event can be identified.
When a rotator cuff tears, the shoulder becomes painful and often weak. Pain often radiates down the arm in the region of the deltoid muscle. Shoulder motion may be lost. It may be difficult to sleep at night and to use the affected arm during the day.
Examination
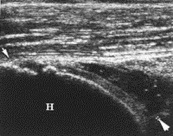 Ultrasound of Rotator
Ultrasound of Rotator Cuff Tear
Clinical findings of rotator cuff tears include signs of mechanical impingement and weakness of the rotator cuff. This can be tested by abducting the arm to shoulder level, bending the elbow, and rotating the forearm internally and externally (Hawkins Test). Pain during this maneuver is consistent with impingement. Alternatively, impingement can be tested by simply elevating the arm above shoulder level (Neer Test). To isolate the supraspinatus, the arm is placed at shoulder level with the elbow extended and the thumb pointing down (internal rotation). Weakness during isolated supraspinatus testing is consistent with a tear of the supraspinatus.
Imaging
A rotator cuff tear is typically confirmed by Diagnostic Ultrasound, Magnetic Resonance Imaging (Figure 1) or at the time of surgery.
 MRI of Rotator
MRI of Rotator Cuff Tear
The thickness of the tear is extremely important. When the tendon does not tear all the way through it is called a partial thickness tear. However, when the tear goes completely through the tendon, it is a full thickness tear.
Full thickness rotator cuff tears will not heal by themselves. Additionally, studies have shown that rotator cuff tears get larger with time, and muscle atrophy that develops while the tendon is torn will become permanent (even after a successful repair). The larger the rotator cuff tear, the more shoulder function is lost.
Interestingly, some patients with rotator cuff tears do not have pain. It is thus possible to rehabilitate the shoulder to help eliminate pain. However, shoulder strength will not improve, and many patients will eventually have pain.
Non-operative Treatment Options
Non-operative management of rotator cuff tears consists of a combination of activity modification, physical therapy, anti-inflammatory medications, and cortisone injections. Studies in the orthopaedic literature have noted that non-operative treatment will help in approximately 60 to 70% of patients. It is therefore often the initial recommendation for patients with minimal demands on their shoulders. Patients with higher demands on their shoulders should be strongly considered for early operative treatment. The best results of rotator cuff repairs are in patients treated early.
Operative Treatment

Surgical treatment of rotator cuff tears involves repairing the rotator cuff to the greater tuberosity where it normally inserts. This section of the greater tuberosity is called the “footprint” of the rotator cuff. Historically, this surgery was performed using a large incision over the shoulder, and often required a temporary detachment of a portion of the deltoid.
With the advancement of arthroscopic surgery, even the largest of rotator cuff tears are now being treated using an all-arthroscopic minimally invasive technique. Most of the recent technological advancements in rotator cuff surgery have been directed at re-attaching the rotator cuff back to the anatomic position where it was torn, completely covering the “footprint” of the rotator cuff.
Several biomechanical studies have concluded that the strongest repair of the rotator cuff is achieved by using a double row method. Double row repairs of the rotator cuff involve placing two sets of attachment on either side of the rotator cuff tendon edge (see figures to right). The sutures repairing the rotator cuff create a web of compression over the tendon, creating the best environment for healing.
 Double Row Repair
Double Row Repair of Rotator Cuff Tear
Results of rotator cuff repairs continue to improve, as technological advancements facilitate arthroscopic repairs of rotator cuff tears of all sizes. With an emphasis on recreating normal anatomical attachment of the rotator cuff, all-arthroscopic double row rotator cuff repairs remain on the cutting edge of shoulder surgery.